

Useful Stories and Pain Relief: On Sarno’s Healing Back Pain
Dr. John Sarno's legacy matters, even if his explanation no longer holds up.

You wake up with back pain, one day, and, dissatisfied by the doctor’s diagnosis ("herniated disk") and prescription (ibuprofen), you start scouring the Internet for alternative explanations.
Whether through startup founder, celebrity endorsement, or online testimonial, you soon come across the writing of the late Dr John Sarno.
Quick facts on Sarno:
Surgeon and Professor NYU School of Medicine
Became convinced most chronic pain was not from tissue damage1
Stopped doing back surgery after observing no consistent benefit
Wrote Healing Back Pain, The Mindbody Prescription, sold millions of copies directly to the public, to the chagrin of much of the medical community2
Successfully treated over 10,000 patients with education rather than surgery3
Sarno passed away in 2017, but he remains the most influential (if controversial) public facing writer on the causes and resolution of chronic pain (especially lower back pain).
I want to argue here that Sarno’s teachings were effective, even as his explanation was incomplete.
Sarno’s books work
This may trigger strong skepticism, but make no mistake: Sarno’s books have resolved the chronic pain of many thousands of people. I have firsthand experience of this, and thousands of credible people with no clear incentive of lying have given long, detailed testimonials. If you’ve experienced persistent pain, you will realize that it is difficult to fool yourself into thinking your pain is gone. For all these testimonials to be wrong would require an extraordinary amount of evidence.
For those that remain skeptical, I invite you to examine this evidence page that I’ve compiled.
Note that I am not claiming that all back pain can be addressed in this way, but rather that simply reading one of Sarno’s books has resolved the pain of tens of thousands of people.
Sarno’s mechanism is vague and incomplete
The diagnosis that Sarno gives to many types of chronic pain is ‘Tension Myositis Syndrome’ (TMS). He elaborates on this in Chapter 3 ("The Physiology of TMS") of Healing Back Pain:
““The physiology of TMS begins in the brain. Here repressed emotions like anxiety and anger set in motion a process in which the autonomic nervous system causes a reduction in blood flow to certain muscles, nerves, tendons, or ligaments, resulting in pain and other kinds of dysfunction in these tissues… This state is known as ischemia—that is, the tissue involved is getting less than its normal complement of blood. This means that there will be less oxygen available to those tissues than they are accustomed to, and the result will be symptoms—pain, numbness, tingling, and sometimes weakness.”
That’s as precise as Sarno gets. For evidence, he cites two papers4 and the success of his methods. I couldn’t find the 1973 Wegner and Fassbender paper, but the 1983 Lund, Bengtsson, and Thorborg paper is about fibromyalgia specifically has a sample size of 18. As for Sarno’s personal experience: history is rife with doctors helping patients without a precise causal explanation.
It’s certainly plausible that ischemia is involved in chronic pain (a 2017 review paper on fibromyalgia5 acknowledges ischemia as one of several plausible mechanisms), but Sarno’s explanation is not a complete theory. “Repressed emotions… set in motion a process” is hardly a mechanism, and is not yet useful for making predictive claims.
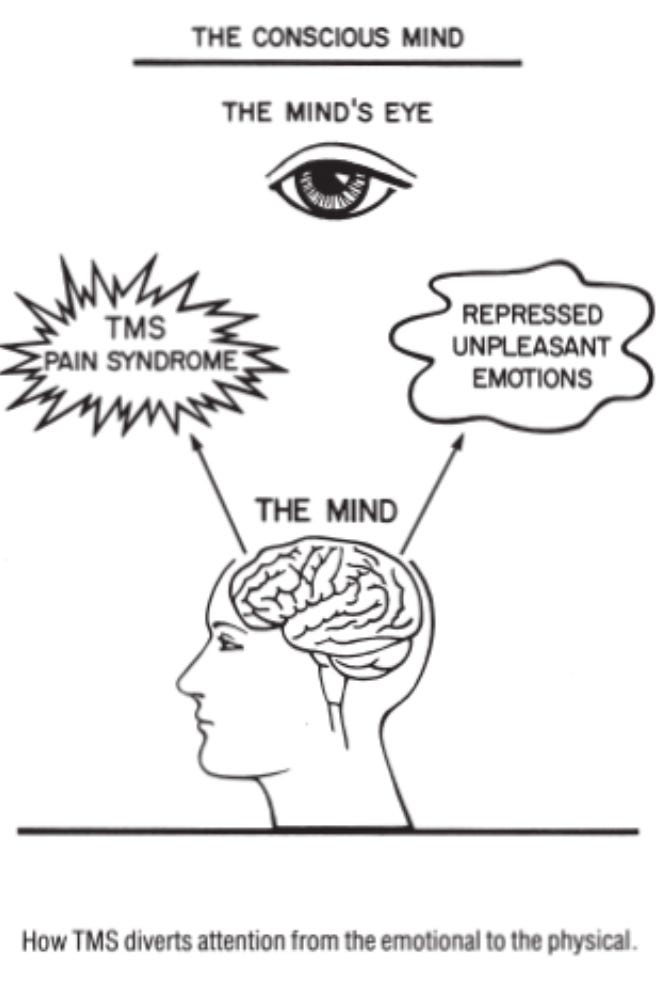
His explanation for how resolution happens is that the ‘conscious mind’, after confronting the repressed unpleasant emotions, no longer has a need to generate pain as a distraction. This explanation is intuitive and useful. I wouldn’t call it wrong, so much as vague and difficult to map onto what we know of the neurobiology of pain.
One important phenomenon that Sarno’s theory would fail to account for is phantom limb pain. Around 80% of amputees experience pain in the limb that has been removed6. In a non-attached limb, there is no blood flow to restrict, so decreased oxygen flow cannot explain the pain.
What is the alternative?
Modern pain science has moved far beyond Sarno’s model of restricted blood flow. In applied clinical research, scientists like Lorimer Moseley have run several experiments demonstrating that you can significantly change someone’s reported pain by altering the associated sound and visual cue7. Their work, alongside Melzack’s neuromatrix theory, is now becoming part of institutional syllabi.
I’ll give a brief account of my favorite theory — which is both biologically plausible and can explain how someone like me can read Healing Back Pain and go from effectively disabled to normal in two weeks.
The mind and body are a predictive system.
The brain does not passively receive sensory information — it creates a controlled hallucination based on prior experiences and expectations. This is well established in visual and auditory processing8, but is true also at an interoceptive level; we also infer the signals within our own bodies.

Pain is more helpful to understand as a control signal generated by the mind9. Under this view, most chronic pain is a persistent misinterpretation of harmless sensation as damage. Chronic pain can be understood as a self-reinforcing pattern: having internalized that ‘pain is damage’, we interpret sensory input through this lens, which is reinforced by our emotions and thoughts. I have a forthcoming paper with much more detail10, but for those curious for specifics, I would point you to Seymour’s 2019 paper.
Sarno's book, in its persuasiveness, caused many people to update their prior expectations from “pain means I am not safe” to “I can be safe even though I have pain”. By convincing patients that there was no structural damage—just a benign process related to emotional factors—he changed low level priors, which dissolved the self-reinforcing pattern. This is how education alone could change something as visceral as chronic pain.
We need more 100 more John Sarnos
To the extent that the control signal account of pain is true, we need hundreds more John Sarnos. Writing to MAHA Moms, WWE fans, people who read Stripe Press, NIH grant reviewers, and of course the class of 2027 MDs. Sarno’s proteges, Howard Schubiner, and David Schechter have done great work; my wish is for these ideas to come forth and multiply.
This is my vision and mission with this newsletter, Debug Your Pain. Through both our teaching and our writing, Tanner and I hope to contribute to this legacy of pain education by updating and adapting these concepts.
Sarno's view that most chronic pain is not from tissue damage is increasingly supported by contemporary pain science. A systematic review by Brinjikji et al. (2015) found that imaging findings of spinal degeneration are present in high proportions of asymptomatic individuals, with disk degeneration present in 37% of asymptomatic 20-year-olds and 96% of asymptomatic 80-year-olds, demonstrating that structural "abnormalities" often don't correlate with pain experiences.
“Nearly every day, he ate lunch alone in the N.Y.U. cafeteria while the other doctors huddled together at their own tables. He wasn’t invited to their cocktail parties. He was not asked to teach his work and was never invited to present at the monthly department meetings.” From NYT.
"At the Root of Back Pain". WholeHealthMD. From the TMS wiki and scroll through the testimonials, I would wager that 10,000 is an absolute lower bound. "Healing Back Pain" has over 8,000 reviews on Amazon "The Mindbody Prescription" has around 3,600 reviews. Considering a 1:100-200 review-to-sales ratio, I’d estimate at least 1-2 million copies have been sold since they were listed on Amazon. This itself would be a lower bound since HBP was released in 1991.
Fassbender, H. G., and K. Wegner. "Morphology and pathogenesis of soft-tissue rheumatism." Zeitschrift fur Rheumaforschung 32.9 (1973): 355-374.; Lund, N., A. Bengtsson, and P. Thorborg. "Muscle tissue oxygen pressure in primary fibromyalgia." Scandinavian Journal of Rheumatology 15.2 (1986): 165-173.
Chapman, C. Richard, and Charles J. Vierck. "The transition of acute postoperative pain to chronic pain: an integrative overview of research on mechanisms." The Journal of pain 18.4 (2017): 359-e1.
Limakatso, Katleho, et al. "The prevalence and risk factors for phantom limb pain in people with amputations: a systematic review and meta-analysis." PloS one 15.10 (2020): e0240431.
E.g. Moseley, G. Lorimer, and Arnoud Arntz. "The context of a noxious stimulus affects the pain it evokes." Pain® 133.1-3 (2007): 64-71.
To experience this firsthand, you might see the audio excerpt in Anil Seth’s TED Talk, or just look at any instance of the Ponzo illusion.
In other words, pain is something your mind does, not what it perceives from the environment. Just like your mind creates the sense of ‘largeness’ for the top bus in the illusion above, the subtle warm irritation in your lower back is created by your mind.
Working title: “Stuck interoceptive priors? An active inference approach to pain chronification”. Sign up to our mailing list to be notified when I release the preprint!